Presented by Monica E. Warner, M.S., R.D., C.D.N.
Research Coordinator, Carcinoid Cancer Foundation, Inc., New York
It is with deep sadness that the Carcinoid Cancer Foundation announced the passing of Monica Warner in August 2009.
This 2008 update includes minor changes to the original lecture from year 2000. It includes results from a survey done in 2005. What we found is that the major recommendations from the original survey are very similar and are therefore as valid today as they were then.
The only truly new update are the Guidelines for Older Adults
However, we find that the best guidelines for people to prevent cancer and patients with cancer are those published by the American Institute for Cancer Research. (AICR)
I am here today to share with you our progress in developing food and nutrition guidelines for persons with carcinoid disease.
As we all know carcinoid disease is not only relatively rare but also very complex from both a diagnostic and treatment perspective as are also the nutrition issues that surround carcinoid disease.
The medical community has made remarkable progress within the past ten years in diagnostic and treatment options but the nutritional support aspects of carcinoid disease are lagging behind. There are specific dietary guidelines for numerous medical conditions such as Diabetes, Heart Disease, Sprue, Kidney Disease, but as you know there is no specific diet for carcinoid patients as of yet, although in our experience many will benefit from adjusting certain components in food.
When giving nutrition advice or, as in this instance, developing guidelines, I looked at various resources, such as general nutrition guidelines for the healthy population, nutrition guidelines for cancer patients, epidemiological studies, clinical studies of individual nutrients etc., and then made a judgment on available evidence: what will PROBABLY help; what will POSSIBLY help and what has INSUFFICIENT evidence?
I must emphasize at this point that these are only GENERAL GUIDELINES since patients with carcinoid may have multiple problems and must be assessed on a case-by-case basis. However, these guidelines are a good base to start with in tailoring your food intake. It is highly advisable that you seek professional advice from a reliable nutritionist that can help you determine what your nutritional needs are and also can guide you in the right direction regarding food and supplement intakes.
I just want to tell you a little bit of how I got involved in looking into nutrition concerns for the carcinoid patient. Besides my practice in Nutrition Consulting, I have been working with my husband for about 15 years, mostly as a medical office manager and administrator for The Carcinoid Cancer Foundation. Very often people with carcinoid disease would come to me and say, “We have so many questions about nutrition and food.” So, by observing and by listening to people over the years, we began to realize there really is a need for people with carcinoid to get information on what foods to eat or not to eat, and what they can do nutrition wise to improve their health and quality of life.
The main goal of this lecture is to help you to choose and adjust among all the foods that you are now eating and like, which foods may be helpful to avoid or decrease symptoms, and which will give you optimal health and help you fight your disease. I hope that at the end of this session you will be able to:
- Assess your current food intake for nutritional adequacy
- Be able to modify food intake to optimize your nutritional status
- Identify foods/substances that may provoke carcinoid syndrome
- Be able to determine supplements that may be beneficial in overall nutrition and well being
It has not been an easy task to put these guidelines together. In researching epidemiological studies, results from clinical trials, and nutrition textbooks, I found more than 7400 medical references for carcinoid. Looking for information about nutrition and diet in cancer, in general, I found over 7300 references. Moreover, when searching for information on diet and nutrition in carcinoid I got no more than four references. Because of the scarcity of information from medical peer review literature, we decided to do a nutrition survey to perhaps begin to see what nutrition related problems and needs the carcinoid population had. In October of 1999, we asked people to fill out a questionnaire for a nutrition survey and received 97 responses.
The information that I am presenting to you today, has been drawn from established guidelines for optimal health, some have been borrowed from diet and nutrition recommendations for general cancer prevention and treatment, and finally from the results of our nutrition survey. Our assumption is that foods or substances in foods that have been found to prevent cancer will also be beneficial in preventing recurrence or progression of the disease.
RESULTS FROM THE NUTRITION SURVEY
Figure 1.
As shown in figure 1, the age at time of diagnosis for carcinoid patients responding to the nutrition survey is between 26 and 81 years of age. The average age is about 52. 62% were females, and 38% males. One of the questions was, what was the year of diagnosis and we found people that were diagnosed as far back as 1974. However, most of the responders were newly diagnosed. I just wanted to share that with you. It is nice for those who were diagnosed in ’1990, ’1999, to see that there are people hanging in there from even as far back as ’1974.
PRIMARY AND SECONDARY TUMOR LOCATIONS
Figure 2.
Figure 3.
In 22%, of the people who completed the survey, no primary tumor was found. 43%, had their primary in the small intestine, 13 % in the lung, colon 5%, stomach 4%, appendix 3%, ovary 1%, pancreas 3%, liver 3%, and 3% in some other sites (figure 2). So that is pretty close to the same distribution as you heard in Dr. Warner’s lecture. Of secondary tumors or metastases 65% had liver metastases and 33% had metastases in the lymph nodes, 14 % metastases lung, and so forth (figure 3)? This just shows you the characteristics of the tumor location.
TREATMENTS RECEIVED AFTER INITIAL DIAGNOSIS
Figure 4.
I also was interested in what type of treatment people have had to see if any of those treatments would have any nutritional implications (figure 4). For example, 79% had surgery of which 55% had some type of intestinal resection, which at times can have nutritional implications. A total of 63% of this group were on Sandostatin and what might be interesting for you to see is that 24 % of the 63% were on the combination Sandostatin and Interferon, 30% were on the long acting drug alone, 28% took long acting with a booster shot, and 18% were taking the regular sub Q. 19% of this group has had hepatic artery chemoembolization and out of that, I think three had just plain embolization. Other types of treatments including chemotherapy, radiotherapy, and so forth were 20%.
In reviewing this information the question was how much of the information could be applied to some form of nutrition related intervention. What I would like to talk to you about is food; how food can help you maintain optimum health, to help in fighting your disease better and improve your quality of life. However, I want to emphasize that food and nutrition manipulation must be looked at as support; complementary to other treatments you receive and not as a cure in itself.
SO, WHAT AND HOW SHOULD WE EAT?
The important point to remember here is that you do not want to think of being on a diet per se but rather look at what you’re eating now, what you like to eat and, with a couple of simple changes adjust your food intake to accomplish the goals we previously discussed.
All points may not necessarily apply to your individual case but I have tried to answer the most commonly asked questions from the nutrition survey.
- Is there a special diet for carcinoid patients?
- What foods or nutritional regime might delay or eliminate the growth of tumors?
- What foods can prevent growth of carcinoid tumors?
- What foods should we absolutely avoid?
- What foods help to improve quality of life?
- What diet should a person with no symptoms be on?
- What regime should I follow to reduce a recurrence of the disease?
GENERAL GUIDELINES
If you would take a meal to the laboratory and have it analyzed, you would find that it contains many nutrients whose names I am sure you are familiar with. I am not going to give you a nutrition lesson but just go over some points of each of these nutrients relevant to patients with carcinoid; in what foods you find these nutrients and how you can adjust them to be as beneficial to you as possible.
Figure 5
You will find that foods contain various amounts of carbohydrates, protein, fats, and water (called Macronutrients =macro for large). These nutrients you can actually see and adjust the quantity in your diet. You can eat more protein, less protein, more carbohydrates, less carbohydrates, and so forth. These nutrients are valuable in the sense that you can control them. Then you have other substances like vitamins, minerals, trace elements, and thousands of other substances (called Micronutrients = micro for small). These nutrients you cannot see, and therefore they are harder to adjust (figure 5).
INCREASE YOUR PROTEIN
1. As Dr. Warner pointed out, in most cases, even in the absence of clinical symptoms (i.e. carcinoid syndrome) carcinoid patients tend to have chronic low levels of Tryptophan (this is an essential amino acid found in complete proteins and is a precursor to serotonin) more than 60 % of Tryptophan may be diverted to the tumors for synthesis of serotonin. Tryptophan is also necessary for the synthesis of other proteins and niacin.
2. In a sense, the term “protein” is synonymous with life, because all living cells contain protein. However, for cancer patients in particular, eating sufficient protein can make an important difference in how quickly and how well they recover as well as in their quality of life. In healthy adults, protein is used to repair tissue, maintain a healthy immune system, and provide energy. Cancer patients often need twice as much protein on a daily basis because of the physical stress that they are under. By this, I do not mean that that a cancer patient needs to eat a 15-ounce steak. There is a formula that nutritionists use to calculate how much a person needs on a high protein diet which is approximately 1-1.5 grams of protein per kilo ideal body weight, which comes out to approximately 0.5 g per pound of ideal body weight for non-weight losing individuals or 0.7g for the person who has lost weight, or 75 to 105 grams of protein for a person who’s ideal body is 150 lb which translates to about 10 or 15 ounces of meat, fish or other protein sources per day. Now, protein, of course, you find in fish, beef, veal, lamb, pork, chicken, eggs, dairy products, and soy products. If you have any questions about this, I will be happy to answer them later on. However, a high protein diet is, very important to help a carcinoid patient maintain optimum health.
CARBOHYDRATES (fruits, vegetables and whole grains) 5-10 servings/day
If you review epidemiological studies, you would find that there is overwhelming evidence that a diet rich in fruits, vegetables, and whole grains (the main contributors of carbohydrates) protect against cancer. Even in clinical trials, researchers find that people who are taking in large amounts of fruits, grains, and vegetables have a lower incident of cancer. You probably are all aware of this, some compounds in these foods such as vitamins and phytochemicals are believed to have cancer protective capabilities. But, once researchers started to analyze these particular individual components like vitamin C, vitamin A, and vitamin E in supplemental form (often in mega doses), the results to were very disappointing. For example supplementing with beta-carotenes by themselves, did not really work to lower incidence of cancer. In addition, in the latest results of colon cancer and a fiber rich diet the results have not been so promising. From this research, we can conclude that identifying THE specific food or component in food that is responsible for lowering incidence of cancer is difficult. Perhaps the credit belongs to the unique COMBINATION OF CHEMICALS in foods and other yet undiscovered components. We just do not have an answer yet to the benefit of individual nutrients in the form of supplements.
Every ten years or so the Academy of Medicine gives out what’s known as the recommended dietary allowances, (RDA) and the Academy is just in the process of publishing the updated guidelines called the Dietary Reference Intake (DRI). There, however, is no convincing evidence that mega vitamin or mineral doses, antioxidants such as vitamin C, where you take 5 gram or 5000 milligram per day, or Beta-carotene, or vitamin E in massive doses will prevent or cure cancer. Therefore, the current recommendations are to get the most of the necessary nutrients from whole foods rather than supplements. Everyday try to eat at least five servings of fruits and vegetables, or better yet seven to ten servings.
An interesting observation in reviewing epidemiological studies is that it may not be bad for a person to occasionally eat the so-called “bad” foods. I am sure you are aware of the supposedly “ bad “ foods. Meat is bad for you, sugar is bad for you, and you should stay away from this and that. In the past, most health conscious people would avoid these supposedly “bad “ foods. But what health professionals are beginning to feel now, is that not that the “bad” foods are the ones that are harmful to you if part of a varied diet; it is rather that, if a person does not take in enough vegetables and fruits, that might be causing the problem. In other words, inadequate intake of fruits, vegetables, and grains seems more detrimental than the inclusion of occasional “bad” foods. So, let us assume you are a steak and potato person. All right, so eat your steak on occasion, but make sure that you have enough of the recommended amounts of vegetables and fruits with your meals too.
FAT- keep intake moderately low (25-30% of total calories)
In general, we recommend that you keep a moderately low intake of fat, as recommended by the American Heart Association and the American Diabetes Association.
For those with carcinoid syndrome with a tendency towards diarrhea, high fat foods will worsen it. Also in patients, taking Sandostatin, digestion of fat may be reduced causing steatorrhea (commonly referred to as “floaties”) and further loss of other nutrients. As a consequence of intestinal surgery, many people have a shortened intestine and, a low fat intake will better control resulting diarrhea.
VITAMINS AND MINERALS IN FOODS
Vitamins, minerals, and trace elements are so minute that you cannot see them. You cannot easily adjust them. You will find them in ALL foods. They sort of come along for the ride in a sufficient well balanced diet. I do not know if any of you tend to eat the same thing day in and day out, such as the same breakfast like toast and orange juice. The key to assure that you get enough essential vitamins and minerals is really to eat a larger variety of foods. The larger the variety of foods the more likely you are to get all the vitamins and minerals that you need. With a risk of sounding redundant, I would like to emphasize that to get the most of these important nutrients in food the recommendation is to EAT A VARIETY OF FOODS.
What about vitamin deficiencies? In some carcinoid patients, particularly in those with weight loss, excess serotonin production from tumors, or low food intake because of poor appetite, could result, even on a well balanced diet, in a Niacin deficiency.
Symptoms of niacin deficiency (Pellagra) are skin lesions; a scaly dermatitis especially in areas exposed to the sun, diarrhea, nervousness, and depression. Since Niacin is manufactured from Tryptophan (an amino acid found in protein), a well-balanced diet high in protein is very important. In addition to protein rich food, supplementation with Niacin (usually in conjunction with other vitamins such as thiamin and riboflavin) is often recommended,
Food sources of Niacin are:
- Meat, Poultry and Fish (40%)
- Grain Products (38%)
- Vegetables (11%)
- Legumes, Nuts, and Soy products (4%)
- Fruits (2%)
The criteria that we use to determine a need for Niacin supplementation (figure 7) is if a person is experiencing weight loss, flushing, poor appetite, or elevated serotonin levels. If these symptoms occur, we then definitely recommend a supplement of Niacin. Again, this emphasizes the importance of a high protein intake, at the recommended level of 0.7g of protein per pound of ideal body weight and a Niacin supplement of about 25 to 50 milligrams twice a day. We have heard of some people who have had problems with flushing even from very low doses of Niacin. Hypersensitive persons may benefit from taking ½ a pediatric Aspirin before each Niacin dose or to use the no-flush version, Nicotinamide.
Figure 6.
OTHER SUBSTANCES IN FOOD
- WATER/FLUIDS
- HERBS
- SPICES
- AMINES; Tyramine, Dopamine, Methylxanthines, Theobromide, Histamine
- SEROTONIN
- PHYTOCHEMICALS
WATER/FLUIDS
Of beverages needed, water is of course essential. The amount of fluid intake recommended per day is the same as in the general population: 2 quarts a day
However. Beverages come in many forms. Some beverages can be provocative in some carcinoid patients such as caffeine containing drinks, alcohol, and carbonated drinks (soda). Water and fluid intakes are especially important for people who have chronic diarrhea. At least two quarts per day and in severe case these fluids should contain important electrolytes, which you can find in drinks such as Gatorade.
HERBS
Regular household herbs contribute not only flavor but also important Phytochemicals.
SPICES
Hot spices that “burn” your tongue, such as pepper, cayenne pepper, mustard can provoke diarrhea or flushing in some people. Mild spices such as cinnamon or nutmeg have not been indicated as triggers. This brings us to the subject of other possible trouble foods:
OFFENDING FOODS
I remember when I first started looking into the issue of symptoms and reactions in carcinoid disease. I realized that not only could a person have a reaction such as flushing and/or diarrhea or carcinoid crisis from emotional as well as physical stress, but also from food. Most medical references mentioned foods as a trigger. Nowhere could I find information on what foods. Now, as a nutritionist, I could not very well tell people to stay away from food. I needed to be a bit more specific. We have found from years of experience that people react to alcohol, hot spices, and high fatty foods. However, on occasion we would get feedback about reaction to other foods. This initiated our interest in a Nutrition Survey. The survey results show that 35% of people had some kind of food reaction (carcinoid crisis), 25% had a reaction to a large meal although we could not specify exactly what kind of reaction. 38% experienced flushing, 34% had diarrhea. 39% of the 97 survey responders reported one or more responses. What foods did they react to? (Figure 7)
Figure 7.
The number one “offender” turned out to be large meals. You know, Thanksgiving, weddings, Christmas, where people tend to eat huge meals. Alcohol came in second. The third one, which I was very surprised about, was tomato dishes, (cooked tomatoes are better tolerated than raw) and the fourth one was fatty foods. Then came coffee and caffeine containing drinks, chocolate, nuts, spicy foods (a surprising eighth place), raw vegetables, pineapple, vinegar, cheese, milk, bananas etc. We do not know what the significance of the least reported foods are like dried fruits, carrots, cabbage, as each were only reported by one single person. To determine what foods may trigger a reaction and therefore might be beneficial to avoid or eat sparingly of, be aware of those foods that people reported most frequently as problem foods. It is important to remember that these foods may trigger attacks, hence affect quality of life, but will not make tumors grow.
AMINES IN FOOD
As we started to take, a closer look at these offending foods, we were curious to see if we could detect what substances in food was causing these reactions. Credit for another discovery about offending foods goes to Dr. Woltering. A couple of years ago, he mentioned, in one of the issues of Ray of Hope, to stay away from foods that contain amines, theobromine, xanthenes, and caffeine. It turns out that many of the foods reported on the survey indeed contain these substances
These substances, vasoactive amines are called pressor amines. They are precursors for catecholamines such as adrenaline, which trigger carcinoid tumors to secrete vasoactive substances, which cause symptoms or carcinoid crisis. Tyramine is the most active of these amines. Another amines found in food are dopamine. Other strongly active vasoactive amines found in food include serotonin and histamine that can cause strong dilation of capillaries, and also cause hypertensive crisis. Reported reactions from these vasoactive amines are acute hypertension, headache, palpitations, tachycardia, and flushing and unconsciousness. Interestingly enough, a lot of these foods, which causes reaction in carcinoid patients, whether it is flushing, diarrhea or both, or even crisis, are the same foods that people who are taking monoamino-oxidase inhibitors are sensitive to. As a general rule, Tyramine and other pressor amines are usually only present in AGED, FERMENTED, AND SPOILED PROTEIN PRODUCTS.
Here are some samples of amine containing foods and beverages:
AMINES IN FOODS (VERY HIGH)
TYRAMINE, DOPAMINE
- Aged cheeses (cheddar, Camembert, Stilton)
- Alcoholic beverages
- Smoked, salted or pickled fish or meat (herring, salami, sausage, corned beef, bologna, pepperoni)
- Any spoiled protein foods (chicken liver)
- Yeast extracts and Brewers yeast, hydrolyzed proteins
- Broad beans, sauerkraut, shrimp paste, some soybean products, miso soup, soy sauce, tofu
AMINES IN FOODS (MODERATELY HIGH)
TYRAMINE, DOPAMINE, XANTHENES, THEOBROMINE
- Caffeine containing drinks, coffee (in large amounts), soda
- Chocolate (in large amounts)
- Some nuts (peanuts, coconuts, brazil nuts)
- Some pizzas, raspberries, banana, avocado
Tyramine content can vary widely from brand to brand.
Amounts eaten also make a difference.
Some of these foods are very high in tyramine and should probably be avoided by people prone to strong reactions, but others are moderately high. Foods that are moderately high in these substances, such as coffee, chocolate, some nuts and pizza can be eaten in small amounts. That means that you do not necessarily have to stay away from this food completely, as long as you do not overeat it. For example, people could probably tolerate one or two cups of coffee, but not fifteen.
If all the foods listed here would be restricted, it would be both tedious and unnecessary. Remember that the consequences of tyramine and other amines are dose related. Simply be careful. Shouldyour favorite foods contain these substances, remember that small amounts may not trigger reactions.
Severe reaction10-25mg Tyramine per meal
Moderate reaction 6-10mg Tyramine per meal
SEROTONIN IN FOODS
One of the most frequently asked questions is “ should I stay away from foods that are high in Serotonin?” This reminds me of the time when I was working as a dietician many years ago and we were trying to treat people with high cholesterol. In the 1960’s, the theory was that, if your blood cholesterols are high, then you have to stay away from high cholesterol foods. Does that sound familiar? Well, as time has gone by we realized that the solution to lowering high cholesterol was not that simple. As we found out the hard way, the strict low cholesterol diets did not lower blood cholesterol levels. The same thing is true about Serotonin in foods. Should we stay away from them? The answer is NO. The only time that you would want to stay away from foods that are high in Serotonin is before and during the collection of the 24-hour urine for the 5-HIAA test.
Why is that? Well, it is believed that Serotonin in foods is broken down into 5-HIAA (5-hydroxyindoleacetic acid, breakdown product of Serotonin) while it is being absorbed through the lining of the intestine and is excreted in the urine as 5-HIAA. Therefore, you do not want to eat a lot of high Serotonin foods before a 24-hour urine because you may get a false positive result.
Below shows results from a study by Dr. Jerome Feldman at Duke University indicating how high Serotonin food intake can affect the urine 5-HIAA test. The normal range of 24-hour urine -5HIAA level is between 2 mg and 8 mg/dl. A person who eats 32 black walnuts could have a urine 5-HIAA level of 59 mg/dl, whereas four bananas, could elevate the 5-HIAA levels to 15 mg/dl.
Figure 8.
Below are samples of foods that are high in Serotonin like certain nuts, plantains, pineapple, banana, kiwi, plums, and tomatoes.
SEROTONIN IN FOODS
Nuts with high Serotonin (> 3 mcg/g)
Walnut Family:
- Butternuts 398 mcg/g
- Black Walnuts 304 ”
- English Walnuts 87 ”
Hickory Family:
- Shagbark 143 mcg/g
- Pecans 29 ”
SEROTONIN IN FOODS
High Serotonin (> 3 mcg/g)
- Plantains 30.0 mcg/g
- Pineapple 17.0 ”
- Banana 15.0 ”
- Kiwi Fruit 5.8 ”
- Plums 4.7 ”
- Tomatoes 3.2 ”
Then you have other foods that are moderately high in Serotonin such as avocado, dates, grapefruit, and some nuts such as almonds, and cashews.
It is important to remember that if you eat large quantities of foods even moderately low in Serotonin it may still affect the 5HIAA urine test.
SEROTONIN IN FOODS
Moderately High (0.1-3 mcg/g)
- Avocados (Haas) 1.5 mcg/g
- Dates 1.7 ”
- Grapefruit 0.9 ”
- Cantaloupe 0.9 ”
- Honeydew 0.6 ”
- Olives 0.2 ”
- Eggplant 0.2 ”
SEROTONIN IN FOODS
Nuts with Moderately Low Serotonin (0.1-3 mcg/g)
- Brazil nuts
- Filberts
- Almonds
- Cashew
- Coconut
- Macadamia nuts
The foods below are very low in Serotonin, some of which are certain berries, apples, and mangos. Even some nuts are low in Serotonin including pistachio, pine nuts, and sunflower seeds.
SEROTONIN IN FOODS
Low Serotonin (< 0.1mcg/g)
- American chestnuts
- Pistachio nuts
- Pine nuts
- Acorns
- Nutmeg
- Sunflower seeds
- Strawberries
- Blueberries
- Raspberries
- Cranberries
- Apple
- Cherries
- Papaya
- Mango
- Pear
- Peach
- Orange
- Lemon
- Lime
- Carrots
- Cucumber
- Lettuce
Finally, you have foods that contain virtually no serotonin such as ham, chicken, fish, rice, potatoes, tea, coffee, and milk.
SEROTONIN IN FOODS
Low (< 0.1 mcg/g)
- Beefsteak (broiled)
- Ham (baked)
- Chicken (baked)
- Fish (broiled)
- Parmesan cheese
- Corn
- Potatoes
- Rice
- Coffee
- Tea
- Milk
- Wheat germ
NOTE: SEROTONIN IN FOODS WILL NOT AFFECT TUMOR GROWTH.
PHYTOCHEMICALS
Natural foods contain thousands of other substances. You have probably heard of Phytochemicals (simply means ”a chemical from plants which may exert profound disease preventive and curative qualities”) such as Beta-carotene, Lycopene, Genistein, Quercitin, Flavonoids, and Curcurmine, just to mention a few. I am not going to go in depth on this subject because of time restraint, but I did want to bring up this subject briefly since a lot of people take some of these as supplements because they have been told that they possess anti-tumor effects. These substances are sold individually in health food stores and now also in pharmacies. The biggest problem with these unknown substances, sold as food supplements, is that they are not regulated. You cannot be sure that what you intend to buy is what you get because there are no quality or quantity controls. Furthermore, there is also a question about how valuable they are taken in the form of individual supplements. Some of them may work, some of them may not, and in large doses, some may even be toxic. We just do not have an answer yet to their effectiveness. The best approach to assure that you get these potentially valuable substances is by eating a wide variety of plant foods.
SUPPLEMENTS, DO WE NEED THEM?
RESULTS FROM NUTRITION SURVEY
Figure 9.
Vitamin Mineral Supplements
The general guidelines for people who need supplements are:
- People with nutrient deficiencies
- People who eat all-plant diets
- People who have diseases, infections or who have undergone surgery that interferes with food intake, absorption, metabolism of nutrients
- People who take medications that interfere with the body’s use of specific nutrients
As a general rule, we advice our carcinoid patients to take one or two multi vitamin/ mineral supplements per day, especially if they have the syndrome, are loosing weight or have had small bowel resection. In addition we supplement with low dose of Niacin taken two times a day (50-100mg per day divided in two doses) in the form of Nicotinamide no Flush Niacin.
The debate of the benefit of larger doses or megavitamin doses has continued over the past thirty years without a factual proof of benefit.
Complementary/Alternative Nutrition Intervention
Figure 10.
Sample of supplements responders are taking:
- maitake extract, green tea extract, soy isoflavone, curcumin, omega 3 fatty acids, 1400 mg/day; MILK thistle extract, 525 mg/day
- BLACK WALNUT, WORMWOOD, CLOVE IN 1997-1998
- Occuplex, BilberryFOR MACULAR DEGENERATION
- SHARK CARTILAGE 2G 2/DAY, SIBERIAN GINSENG ROOT 400 MG/DAY, MILK THISTLE 200 MG DAY, COENZYMEQ10 120 MG/DAY
- PURE SQUALENE, 2000 MG, SHARK CARTILAGE 1500MG/DAY
- St John WORTS 0.3% 300mg 1/day
- RECENTLY BEGAN TAKING ST. JOHN’S WORT
- shark cartilage 74 grms, 8 capsules IP-6 and Inositol (to enhance NATURAL KILLER cell activity), 6oz Essiac tea.
- All of the above are per day.
- Essiac Tea, MILK THISTLE, GREEN TEA
- FISH OIL, ESSIAC PRO-ESSENCE, MILK THISTLE
- 1 Saw Palmetto 160 mg. – Thrice a day 1 Thisilyn (milk thistle extract) softgel – Thrice a day
- 2000MG SOY, COENZYME 10, GREEN TEA,
- Olive-oil 10 ml /day
- FLAX OIL; COENZYME Q 10 100-200;BORAGE OIL 1000MG; LUTEIN; LYCOPENE; TOCOTRINOLS 50MG;
- SQUALENE 500 MG; AMBROTOSE 1/4-1/2 TEASPOON; KYO GREEN 1 TBS; SPIRAZYMES
- (DIGESTIVE ENZYMES) 2/DAY W/MEALS; MILK THISTLE 500 MG; GREEN TEA 470 MG; GARLIC 600 MG;
- TURMERIC; TAURINE; MSM; QUERLETIN; BROMELAINE; ECHINACEA
- ECHINECEA ROOT – 500mg, 4/DAY, GINKO BILBOA 50 mg, 1/DAY
- kyolic garlic 2 capsules/day
- ESSIAC TEA
- CELL FORTE IP6 800 MG, SHARK CARTILAGE, NSC 100 BETA GLUCANS 10 MG, GREEN TEA, ESIACA TEE
- MILK THISTLE 200 MG
- COENZYMEQ 10, KYOLIC (GARLIC) KYO GREEN 3 TABLETS, GLUCOSAMINE 1000, FLORESCENCE
- GREEN TEA 2-3/Day
- SHARK CARTILAGE
- ONE CAN OF BOOST A DAY
- PAU D’ARCO
Some of these substances often referred to as Complementary Alternative Medicines (CAM) are proven beneficial such as Boost, Omega-3 Fatty Acids, green tea, and some herbal medicines. Other substances such as shark cartilage, megavitamins, individual Phytochemicals, and some herbal remedies are highly questionable and can be outright dangerous. For example it is not advisable to take garlic, kava-kava, Ginkgo Biloba prior to surgery because of their blood thinning properties.
Many do not share with their doctor that they take these substances. We urge you to do so for several reasons. If something is working for you let him know so that other patients may benefit. Additionally you and your physician need to be aware that many alternative substances or therapies may have harmful side effects especially if you are taking medications.
My former professor at TC Columbia University Joan Gussow says: “It is harder to hurt yourself with foods than with supplements. Concentrating anything in food be it Vitamin C or Beta-carotene, Vitamin E etc increases the likelihood of mistakes”.
Be Cautious and Skeptical
“Operation Cure All” Targets Internet Health Fraud
The advice below comes from Federal Trade Commission’s ongoing federal and state campaign to target dubious health claims and health fraud on the Internet. They are trying to stop websites that promote supplements that offer miracle cures. They often use sophisticated Internet techniques to deceive consumers such as metatags and hyperlinks.
HERE’S WHAT YOU NEED TO KNOW
Typical signs of fraudulent claims include:
- Products advertised as effective against a wide range of ailments
- Use of terms like scientific breakthrough, miraculous cure, ancient remedy, etc.
- Impressive sounding terminology to disguise a lack of good science
- Claims the government or the medical profession have conspired to suppress the product
- Testimonials instead of facts and figures
- Product availability from only one source
Keep this list handy, and consult it when you learn about the latest “miracle” before you reach for your credit card.
SUMMING UP GENERAL DIETARY GUIDELINES
(From the American Institute for Cancer Research-AICR)
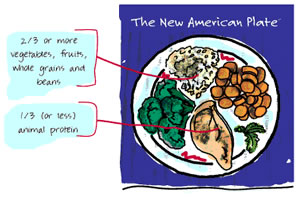
For description of the New American Plate (click here)
You may question yourself, am I eating okay? Use this guide as a baseline to determine if you need to change your current intake. The New American Plate is a good tool to use when you want to determine how well you are eating. You may be pleasantly surprised to find that you are doing just fine. In other words, if it is not broken do not change it. This type of assessment will also tell you whether you might need to increase or decrease some types of food. Your best defense is to start with a well balanced diet and then, as needed, make adjustment in food intake and supplements to your individual needs.
SPECIAL CONSIDERATIONS
Figure 12.
Our nutrition survey (Figure 12) clearly pointed out some of the problems that people are having in spite of medical treatments. Currently only 14% of our responders have no symptoms, 45% reports flushing, 51% diarrhea, 33% abdominal pain, 51% gas and bloating, 21% weight loss, 8% skin rash, and 20% nausea. The major complaint was fatigue and weakness with (60%).
Even though some of these problems can be improved with nutrition intervention, it is very important to FIRST determine what causes them. Not all problems are food related. In addition, there is no single diet that will do all that we would like it to do for everyone. Foods behave differently in different people and may actually have opposite effects in different people. For example, fatigue can be caused by poor sleep, low blood counts, side effects of medicines and depression, which eventually may lead to poor food intake.
Diarrhea can be caused by tumors secreting serotonin, as a result of small bowel resection, response to medication, chemotherapy or sensitivity to certain foods.
Sandostatin can cause a form of diarrhea called steatorrhea, and you know that alcohol and certain foods such as high fat foods or hot spices can also create a problem.
For nausea and vomiting, we must determine the cause. Chemotherapy, stomach ulcers, intestinal obstruction, and drug allergy just name a few, can all cause nausea and vomiting. In general, small feedings of low residue (low fiber), bland or liquid diets may be helpful.
For gas and bloating, again, it is essential to determine the underlying cause. Treatment will depend on it. To adjust food intake may not necessarily be the first thing to do. For example in lactose intolerance, you need to avoid lactose. If Sandostatin is the cause, taking pancreatic enzymes may help. If a person is taking Sandostatin SQ, inject it in between meals. Small frequent meals and fluids between meals are also helpful. Gas and bloating can somewhat be reduced by avoiding gas forming food such as from the cabbage family, onions, carbonated beverages, dried beans, strong cheeses, asparagus, melons, eggs etc.
As you can see it is indeed a very complex process to determine nutrition guidelines for carcinoids and any dietary advice must be tailored to each individual to address his or her particular problem. Below you will find examples of ways to tailor food and supplements in various situations.
CASE STUDIES
Case Study 1
- Age 50
- Newly diagnosed Lung carcinoid
- Lobectomy, no lymph node involvement
- No evidence of metastases
- No symptoms
Nutritional Recommendations
- Well balanced diet with an emphasis on grains, fruits and vegetables (5-10/day)
- Moderate protein and fat intake.
The “New American Plate” by the American Institute of Cancer Reserach (AICR) guideline is a good and user friendly plan to follow.
The New American Plate How it works.
Case Study 2.
- Age 42, Male
- Diagnosed five years ago
- Surgical resection of small intestine due to intestinal obstruction.
- At that time; Small bowel resection (50cm of ileum) Multiple tumors largest 4cm. No symptoms, no mets
- No post surgery treatment. Surveillance only
- Now; symptoms of intermittent flushing and diarrhea
- Octreoscan positive for liver mets, with increasing neuroendocrine markers.
- Starting on Octreotide ( in the US called Sandostatin )
Nutritional Recommendations
- High protein diet(1.5 g/K g= 6-9 oz of protein/day, from any animal source depending on body weight)
- Low fat (<25% of total calories)
- Encourage >5 servings of fruit and vegetables
- Multi vitamin/mineral supplement 2/day
- Niacin supplement 25-50mg 2 /day
- Avoid large meals and possible offending foods, such as amine containing foods, alcohol, spices etc.
Case Study 3
- Age 67, female
- Known liver metastases for 10 years. Primary not found.
- Occasional symptoms of flushing and diarrhea
- Has had three hepatic artery chemoembolizations
- On Sandostatin for 7 years
- Now on combination Sandostatin-Interferon treatment
- 30 lb weight loss over past 6 months
- Poor appetite
- Gas and bloating
- Heart palpitations
- Diarrhea still not totally under control
Nutritional Recommendations
- Small frequent meals
- If fats are tolerated, then higher fat
- High protein and carbohydrates
- Drink plenty of liquids between meals rather than with meals.
- Multivitamin/mineral supplement 2/day
- Niacin supplement 25-59 mg 2/day
- Omega-3 fatty acid supplement
Food supplement such as Boost, Ensure etc.
Consult with registered dietitian ( RD ) to taylor diet to your specific problem.
SUMMARY
IF NO SYMPTOMS
Follow The American Institute of Cancer Reserach (AICR) nutrition guidelines with an emphasis on vegetables and fruits. (ten servings per day)
IF ONE OR MORE SYMPTOMS (THE CARCINOID SYNDROME)
- High protein, low fat foods
- Supplements: low dose Niacin and Standard one a day multi- vitamin/mineral 2/day
- Avoid or minimize intake of foods that may provoke or aggravate symptoms, such as alcohol, spicy and high fat foods, amine containing foods and large meals.
- If you are taking supplements or alternative remedies, let your physician know. Some supplements may interact with medications and be harmful.
- Keep in mind to tailor food and supplement intake to your specific needs and/or problems.
At this time, it is not known whether any dietary manipulation will affect the clinical course of cancer (it will not increase or shrink tumors or cure the disease). HOWEVER, a well-nourished person is less likely to develop complications and will be better able to cope with treatment for the disease. In the case of carcinoid patient, avoiding certain foods that may aggravate symptoms and provoke a carcinoid crisis will surely improve quality of life.
FAMILIAR PACKAGES
“Nutrients and other nonnutritive substances relevant to health are readily available in familiar packages called fruits, vegetables, legumes, grains and animal products and they come in concentrations and combinations with which humans have had a long cultural familiarity” “ Joan Gussow”
What can we conclude from these evaluations?
FOOD IS STILL THE BEST SOURCE OF NUTRIENTS.
WHOLE FOODS ARE BETTER THAN ISOLATED SUBSTANCES BECAUSE OF POSSIBLE SYNERGISTIC EFFECT PLUS FACTORS IN FOODS THAT WE DO NOT KNOW OF.
Your take home message is
FOOD FIRST Thank you

