The Commitment to Courage
Ashley is a United States Marine.
She had served all over the world, facing hazardous situations in combat and fighting for our freedom.
But she wasn’t prepared for the battle she’d have to fight next.
In 2021, she was diagnosed with a neuroendocrine tumor after almost a decade of symptoms — but only because of the research she did herself and the dedication to being her own best advocate.
She continues to lean on the USMC core values of honor, courage, and commitment to ensure she has the best quality of life for herself and her family.
Luncheon with the Experts continues

We are excited to present the upcoming 2024 Luncheon with the Experts schedule via Facebook LIVE taking place on the 1st and 3rd Thursdays of the month from 12:00pm til 1:00pm Eastern Time.
Join us Thursday, April 18th, at 12PM ET, for the next episode of “Luncheon with the Experts” Facebook Live event! Our featured guest will be NET expert M. Bassam Sonbol, MD.
Susan G. Warner, MD, is a Hepatobiliary and Pancreas Surgeon at the Mayo Clinic in Rochester, MN. She is a leader in several professional societies, and has built an international reputation as an emerging leader in academic surgery. Her research interests include clinical applications of oncolytic viral therapies, the biopsychosocial perioperative patient experience, and optimization of minimally invasive surgery platforms for hepatopancreatobiliary surgery. Dr. Warner aspires to “maximize the Mayo Clinic’s multidisciplinary management of NET patients, including appropriately aggressive surgical management when feasible.“
If you have any non-case-specific questions, you are welcome to pose them during the presentation and our guests will try to answer them LIVE! This Facebook Live event will be hosted by B. Rain Bennett a longtime CCF filmmaker and dear friend of the NET community. We hope you can join us! #LetsTalkAboutNETs
If you do not have Facebook, we will also be streaming LIVE on YouTube. Please visit our YouTube channel for past shows you may have missed or that you may want to watch again. To receive notifications of all new videos on our YouTube channel, CLICK LIKE, SUBSCRIBE and HIT THE BELL to receive notifications each time a new video is uploaded.
Latest News
RARE DISEASE DAY 2024
Raising awareness and generating change for the 300 million people worldwide living with a rare disease, their families and caregivers. Visit https://www.rarediseaseday.org/ to learn how you can participate.

Congratulations to Lisa Yen, Director of Programs and Outreach at LACNETS, who was recently featured in ShoutOutLA.
“Hi Lisa, let’s start by talking about what inspires you?
Helping others
Ever since I was a little kid, I wanted to make a difference in the world. At the age of 16, I felt called to be a nurse. I loved working as a cardiac ICU nurse for a couple years and helping people recover after suffering a heart attack or recovering from open heart surgery. I then spent 2 months in a hospital in rural Kenya when I witnessed the challenges of accessing even the most basic medical care. This prompted me to return to school to become a nurse practitioner. I absolutely loved being a NP hospitalist. I loved being able to make a meaningful impact on those who were critically ill. Unfortunately, my world was turned upside down when my husband was suddenly and unexpectedly diagnosed with advanced neuroendocrine tumor (NET or neuroendocrine cancer). While I continue to support him in our journey with this uncommon cancer, I am inspired to help others like him to ease their suffering and help them be able to thrive despite living with cancer.”

Alira Health Partners with CCF and LACNETS to Help NET Cancer Patients Take Control of Their Healthcare Journey
Partnership Empowers Patients with Mobile Platform Providing Critical Patient Support
Framingham, Mass., June 29, 2023 — Alira Health, a global advisory and clinical research firm whose mission is to humanize healthcare and life sciences, announced today the addition of the Learn Advocate Connect Neuroendocrine Tumor Society (LACNETS) to accompany its partnership with the Carcinoid Cancer Foundation (CCF) in supporting those living with NET.


LACNETS & CCF Partner to Provide Support

The Carcinoid Cancer Foundation (CCF) and Learn Advocate Connect Neuroendocrine Tumor Society (LACNETS) are excited to announce a partnership to provide a Support Line for those affected by neuroendocrine tumors (NETs).
The Support Line provides guidance, resources, and referrals to NET patients or their loved ones. The new partnership allows both organizations to leverage each other’s complementary programs and expertise to help NET patients and caregivers around the world.
As one of the most recognized NET-related organizations in the US, CCF receives many inquiries for support from patients and caregivers every year. LACNETS, with its close ties to the patient and healthcare community, is poised to provide the best support possible.
This partnership formalizes LACNETS’ Support Line, which will now provide support to those contacting CCF in addition to direct inquiries. The Support Line is a comprehensive addition to the current range of NET educational programs, advocacy tools, and support groups provided by LACNETS.
To receive support, patients or caregivers can fill out a questionnaire available at www.LACNETS.org/supportline. The answers help LACNETS direct the patient or caregiver to the most relevant informational resources, introduce them to others with a similar diagnosis or treatment plan, or NET experts specializing in their area of inquiry.
Big news from our friends at Pheo Para Alliance which includes NET Specialist and previous Luncheon with the Experts guest, Dr. Karel Pacak!

Dr. Karel Pacak will be the new Chair of the Pheo Para Alliance Medical Advisory Board. The Medical Advisory Board is comprised of 11 medical researchers/clinicians from North America, Europe, and Great Britain, who are all experts in pheochromocytoma and paraganglioma, in addition to a handful of patient representatives who serve on the committee. As part of his responsibilities, Dr. Pacak will also serve on the Pheo Para Alliance Board of Directors.
Dr. Pacak is Senior Investigator for the Section on Medical Neuroendocrinology, NICHD/DIR at the NIH. He is an internationally recognized leader in the study of pheochromocytoma and paraganglioma. He has published over 300 articles on pheochromocytoma/paraganglioma and has authored several books and book chapters. He also has been a frequent and popular contributor to the Alliance’s educational webinars, as well as graciously responding to individual patients seeking his advice. You can read more about Dr. Pacak’s experience here.
CCF Turns 55!
RARE DISEASE DAY 2023
Raising awareness and generating change for the 300 million people worldwide living with a rare disease, their families and caregivers. Visit https://www.rarediseaseday.org/ to learn how you can participate.
A Rare Disease Day Story from a NET Patient!

Dr. Katie Dexter is a PCD and Lung Carcinoid patient. This is her story of navigating not one, but TWO, rare diseases. Watch interview by Rain Bennett a longtime CCF filmmaker and dear friend of the NET community. Watch here.
Making History: Michelle Kang Kim, MD, PhD, is Cleveland Clinic’s First Female Chair of Gastroenterology
The appointment of Michelle Kang Kim, MD, PhD, as Chair of Cleveland Clinic’s Department of Gastroenterology, Hepatology and Nutrition is groundbreaking in several ways. Dr. Kim is the first woman to hold that position at Cleveland Clinic, and she is among the fewer than 10% of gastroenterology division chiefs nationally who are female. Dr. Kim is an expert in neuroendocrine tumors. READ MORE
New Natural History Study of Neuroendocrine Tumors and Neuroendocrine Carcinoma Opens at the National Cancer Institute
 You can help physicians and scientists learn more about neuroendocrine cancer in order to develop future treatment options. A new clinical study, sponsored by the National Cancer Institute (NCI), has just opened and is looking to recruit and follow neuroendocrine neoplasm (NENs) and adrenocortical carcinoma (ACC) patients for a period of ten years in order to learn more about these uncommon cancers. Tissue Procurement and Natural History Study of Neuroendocrine Neoplasms (NENs) Including Adrenocortical Carcinoma (ACC), with principal investigator Jaydira Del Rivero, MD, is a national and international study. READ MORE
You can help physicians and scientists learn more about neuroendocrine cancer in order to develop future treatment options. A new clinical study, sponsored by the National Cancer Institute (NCI), has just opened and is looking to recruit and follow neuroendocrine neoplasm (NENs) and adrenocortical carcinoma (ACC) patients for a period of ten years in order to learn more about these uncommon cancers. Tissue Procurement and Natural History Study of Neuroendocrine Neoplasms (NENs) Including Adrenocortical Carcinoma (ACC), with principal investigator Jaydira Del Rivero, MD, is a national and international study. READ MORE
World’s 1st Distinguished Professorship in Neuroendocrine Tumor Research at UK Markey Cancer Center
Very exciting news from the UK Markey Cancer Center! The University of Kentucky Markey Cancer Foundation received a $1 million gift to create the world’s first distinguished professorship in neuroendocrine tumor (NET) research.
The Amanda W. Lockey Foundation has given the gift in support of UK Markey Cancer Center medical oncologist Lowell Anthony, MD, a specialist in NET treatment. The distinguished professorship in neuroendocrine tumor research will support Dr. Anthony’s work by allowing him and his team to focus on clinical and translational research and the development of a radiotherapeutic program. READ MORE
News for US Veterans with Lung NETs
For US veterans with typical and atypical lung neuroendocrine tumors – the VA has added several conditions to the list of presumptive illnesses related to military service, including lung carcinoid. With appreciation to all our veterans for your service. https://www.fedweek.com/armed-forces-news/va-adds-to-list-of-presumptive-diseases/
Unique Opportunity for Neuroendocrine Tumor Patients
For many neuroendocrine cancer patients, access to physicians who specialize in this disease is challenging or simply not possible. The National Cancer Institute, NCI, is offering neuroendocrine tumor (NET) patients a unique opportunity to have a multidisciplinary tumor board review of their medical records and make recommendations about NET treatment options. READ MORE
Neuroendocrine Tumor Information in 10 Languages

Did you know that the International Neuroendocrine Cancer Alliance (INCA), has free, NET info packets in 10 languages? Click here to select your language and download the factsheets: https://incalliance.org/net-info-packs/. The Carcinoid Cancer Foundation is proud to be a founding member of INCA.
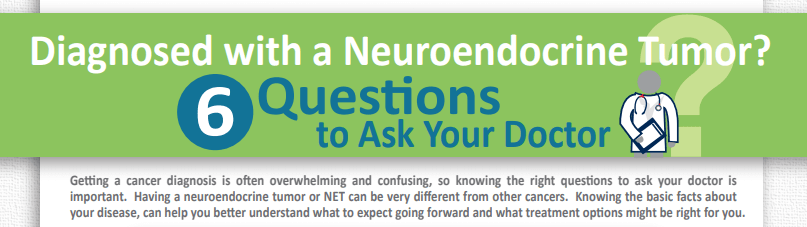
CCF Infographic: 6 Questions to Ask Your Doctor
Have you or someone you love been diagnosed with a neuroendocrine tumor or carcinoid cancer? It can feel like a daunting task to figure out next steps and doctor appointments may be overwhelming. You can help yourself or support a loved-one by learning about the disease and preparing yourself for doctor visits. The first visit may be the most challenging, so It’s important to arm yourself with relevant questions. Here we provide you with six questions, specific to neuroendocrine tumors, to ask your doctor. Click here to download the infographic.
Guide to Understanding Carcinoid Syndrome
Know the signs and symptoms — skin flushing, diarrhea, heart racing . . . it could be carcinoid syndrome! How is it diagnosed, what are the treatment options, what questions should you ask your healthcare provider? Read more in Guide to Understanding Carcinoid Syndrome, from Health Monitor and the Carcinoid Cancer Foundation: https://www.carcinoid.org/wp-content/uploads/2015/10/Carcinoid-Syndrome-Guide-to-Understanding.pdf.
Reaching Those Who Are Still Undiagnosed
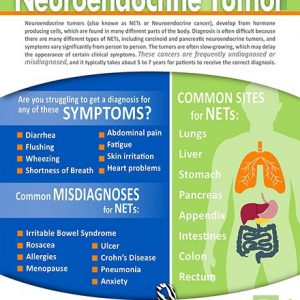 To combat statistics showing that it often takes 5 to 7 years for patients to receive the correct diagnosis of a neuroendocrine tumor (NET), the Carcinoid Cancer Foundation has partnered with Advanced Accelerator Applications to create an infographic — Could You Have a Neuroendocrine Tumor— listing common symptoms and misdiagnoses. Please share this broadly in hopes of helping others get the proper diagnosis more quickly. Download the infographic here.
To combat statistics showing that it often takes 5 to 7 years for patients to receive the correct diagnosis of a neuroendocrine tumor (NET), the Carcinoid Cancer Foundation has partnered with Advanced Accelerator Applications to create an infographic — Could You Have a Neuroendocrine Tumor— listing common symptoms and misdiagnoses. Please share this broadly in hopes of helping others get the proper diagnosis more quickly. Download the infographic here.